FN
255: Introduction to MNT
Teresa (Snyder) McFerran, MS, RD
Health Professions Division
Lane Community College
Eugene, Oregon
Unit 1 Preparations, Chapter 1
Nutrition and Health: Overview
Unit 1 Orientation
Quiz DUE before midnight (11:55 pm) SUNDAY, October
6th
Unit 1 Study
Questions DUE before midnight (11:55 pm) SUNDAY, October
6th
WELCOME to FN 255! Although
this is a fully on-line class, and we will not be meeting
face-to-face during the term, I want you to know that my goal is
to guide you through this course as if I were sitting right next
to you. If questions or concerns come up please take a deep breath
and re-read the material, and maybe skim the Syllabus, before
allowing yourself to become flustered. Once you have taken a deep
breath and re-read the material please consider re-starting your
computer (if this applies) or taking a short five-minute break. If
you are still confused feel free to contact me through our Moodle
messaging system or post your question(s) in our weekly forum. I
would highly encourage you not to wait until the last minute to
submit assignments so you have ample time to resolve any possible
road bumps that may arise. Best wishes and I look forward to
getting to know you as the term unfolds!
UNIT OBJECTIVES
After reading the assigned reading, filling out the Orientation
Quiz Questions, filling out the Unit 1 Outline, participating in
the "Forum Week 1", and
completing the Orientation Quiz AND Unit 1
Study Questions on Moodle, you will be able to:
- Know how this course is organized and where to find the
activities and assignments for each week.
- Communicate with other students in this class and gain
confidence to in our online learning environment.
- Discover due dates for activities in this class, plan
your time commitment accordingly, and set yourself up for
success in this class.
- Define the term "medical nutrition therapy" and
understand some of the common settings where MNT takes place.
- Understand the impact of cultural influences on nutrition
and the importance of cultural competency.
- Review some of the basic principles of nutrition in order
to be able to set MNT goals for a variety of health conditions
throughout the term.
RESOURCES
- Unit 1
Preparations (this document)
- Mosby's Pocket Guide
Series Nutrition Assessment and Care, Ch 1: Nutrition & Health
pp. 3-40
- Reading Calendar (above Week 1 in Moodle)
- Syllabus (above Week 1 in Moodle)
- Merriam webster medical dictionary: http://www.merriam-webster.com/
(select "medical")
- Please use the online medical dictionary to look up any
terminology you may not understand as you are reading the
text.
WEEKLY FORUMS:
Each week, there will be a FORUM that will allow you to post any questions you have about the
lecture or materials covered as well as allow the instructor to
post any changes or corrections
that need to be communicated.
A study question will ask if you participated at least once in this week's
forum BEFORE Friday at 5pm. (Refer the syllabus for additional
details and note that starting next week two forum postings
are required each week.)
FORUM WEEK 1: (Go to our
Moodle classroom and click on "Forum Week 1" to participate.)
- "Introductions": Briefly introduce yourself by
telling us were you grew up, what subject you are studying,
and briefly explain anything about your life right now you'd
like to share, such as your major/career goals,
hobbies/interests, etc. Make sure to include how long it has
been since taking either FN 225 or 105 and what prompted you
to enroll for this course.
-
"Student Questions": Do you have any questions
about the Unit 1
Preparations? Please post your questions/concerns in the
forum for others to be able to respond.
- "Online Success": Since this is an online class,
without a defined time for lecture, it may be a challenge to
find time during your busy week to complete the Unit
Preparations, Case Studies, and SQ (Study Questions). How will
you find a routine time, if you think that's important? If
you've taken an online class before, what wisdom can you
share? If this is your first online class what are your
fears/concerns and how have you already started overcoming
them?
-
"Cultural Competency": Based on the list of ways
in which you can seek out opportunities to develop
culturally competent skills in the Unit Preparations this
week, what ideas seems most practical for you to develop at
this time?
- "Health": How do you personally define the word
"health" or "healthy"? The Word Health Organization (WHO)
defines health as a "state of complete mental, physical, and
social well-being, not merely the absence of disease or
infirmity". How is this definition similar and different than
your definition for health?
-
CORRECTIONS / CLARIFICATIONS: (Please check our weekly
forum for additional corrections and clarifications.)
Notice what your syllabus says in the "Editing Profile" section
for disabling your email
address if you would rather not get messages in
your personal email regarding this class.
Unit 1 Preparations, Chapter 1
Nutrition and Health: Overview
Print and
complete Unit 1 Outline
in Moodle while you are viewing Unit 1 Preparations (this
document) online.
Unlike the Orientation Quiz questions above, the Unit Study
Questions will be based on the answers you obtain from filling
in ALL of the blanks in your outline and checking out the
links for the Unit 1 Preparations below. In other words, you
will not
receive a copy of the actual SQ (study questions). Filling out
the unit preparations outline is the best way to prepare for
the SQ, and considering all quizzes are timed, you will not
have ample time to complete the quiz if the Unit Preparations
are not completed first.
The following topics will be covered this week:
I. Medical Nutrition
Therapy Defined
II.
Cultural Influences on Nutrition and Cultural Competency
III. Nutrition Review
IV. Chapter 1: Nutrition & Health Overview
I.
Medical Nutrition Therapy Defined
Considering the title of this class is Introduction to Medical
Nutrition Therapy, it's important that you can define the term
medical nutrition therapy. The following are a few definitions:
-
Page 281 of our Mosby text states that "acute and
chronic illnesses are treated in a variety of settings,
including acute care hospitals, rehabilitation centers,
extended care facilities, clinics, offices of private
practitioners, and patient's homes. Whatever the setting,
however, nutrition care is an essential part of treatment.
In recognition of its importance, assessment, planning, and
nutrition care of medical, surgical, and emotional
conditions are referred to as medical nutrition therapy."
-
A textbook commonly used by nutrition majors when
studying MNT defines medical nutrition therapy as "the use
of specific nutrition interventions to treat an illness,
injury, or condition" (Krause's food, nutrition and diet
therapy, 11th edn, L.K. Mahan, S. Escott-Stump, p. 496).
-
The Academy
of Nutrition and Dietetics, or AND, defines MNT as
“nutritional diagnostic, therapy, and counseling services
for the purpose of disease management which are furnished by
a registered dietitian or nutrition professional...” (source
Medicare MNT legislation, 2000). MNT is a specific
application of the Nutrition Care Process in clinical
settings that is focused on the management of diseases. MNT
involves in-depth individualized nutrition assessment and a
duration and frequency of care using the Nutrition Care
Process to manage disease.
-
The Centers
for Medicare and Medicaid Services, or CMS, recognizes
that "nutrition and diet play an important role in helping
people with certain diseases manage their health. For people
with diabetes or renal diseases, proper
diet and nutrition can help prevent and reduce complications
from their conditions. Medicare covers medical nutrition
therapy services for people with diabetes or renal diseases
to help them manage their conditions."
Considering CMS provides coverage for MNT for people with certain
diseases, it seems pertinent to recap the ten leading causes of
death in the U.S. (causes in bold indicate that the cause of death
is related to nutrition):
* Heart
disease
* Cancers
* Strokes
* Chronic lung disease
* Accidents
* Diabetes
mellitus
* Pneumonia and influenza
* Alzheimer's disease
* Kidney disease
* Blood infections
II. Cultural
Influences on Nutrition and Cultural Competency
Some of the commonly cited reasons for needing
culturally competent health care individuals include the
following:
- demographic diversity and projected population shifts
- increased utilization of traditional therapies
- disparities in health status of various racial/ethnic
groups
- under representation of health care providers from
diverse backgrounds
Merriam-Webster Dictionary defines culture as "... the integrated pattern of human
knowledge, belief, and behavior that depends upon man's capacity
for learning and transmitting knowledge to succeeding
generations." Therefore, culture is not something we are born
with, but rather it is learned and passed on from one generation
to the next. Culture encompasses more than simply race or
ethnicity because it is a shared system of values, beliefs,
attitudes, and learned behaviors. For example, dress, family
structure, language, and food habits often indicate one's culture.
Below are a few pictures that were taken while my colleague's
husband lived in Japan. The first picture shows the traditional
attire that is worn for kyudo, or Japanese archery. The second
picture was taken at the end of a tea ceremony, or chakai, and the
women are all adored in kimonos. The next picture is of me taking
shodo or calligraphy lessons in Japan, and the last picture is of
dango, which are Japanese dumpling made from rice flour and is
often served with green tea.




Every decade a census of the United States is conducted. According
to the U.S. Census 2010, 308.7 million people live in the United
States. The categories used in the most recent census included
white, black or African American, American Indian and Alaska
Native, Asian, Native Hawaiian and other Pacific Islander, and
"some other 'race.'" Most of the respondents who answered
"some other race" were Hispanic or Latino. Note: Clearly, there
are many subgroups within each of these categories.
According to the U.S. Census Bureau, "between 2000 and
2010, the Hispanic population grew by 43 percent, rising from 35.3
million in 2000 to 50.5 million in 2010. The rise in the Hispanic
population accounted for more than half of the 27.3 million
increase in the total U.S. population."
The expected changes in the nation's demographic makeup in race
and age categories have been cited numerous times as reason enough
for health professionals to pursue personal competence in cultural
knowledge. It is projected that by 2050 Latinos will triple to become the largest
minority group and the percentage of Asians will nearly double. By 2065 Non-Hispanic
whites will most likely be a minority
group.
The table below shows the approximate distribution of
race/ethnicity of the overall U.S. population, based on the 2010
U.S. Census:
Race/Ethnicity
|
% of U.S.
Population, 2010
|
White
|
72%
|
Hispanic or Latino
|
16%
|
| Black or African
American |
12%
|
Asian
|
5%
|
American Indian and
Alaskan Native
|
<1%
|
Native Hawaian/Other
Pacific Islander
|
<1%
|
2010 U.S. Census data
The U.S. Census Bureau website 2010, American Community Survey,
includes a breakdown of the demographic characteristics of Lane
County, Oregon:
POPULATION OF Lane County: In 2010, Lane County had a total
population of 351,715. Fifty-one percent were female and 49
percent were male. The median age was 39 years. Twenty percent of
the population was under 18 years and 15 percent was 65 years and
older.
Please go to the following link (http://factfinder.census.gov/)
and enter Lane County, Oregon. Based on the information, answer
the questions in your Outline.
Many agree that the US population is currently more like a "salad bowl" rather than a
"melting pot." A salad may contain many ingredients, and blend
into a harmonious whole, but each ingredient retains its unique
taste and texture.
However, it is not enough to simply recognize and accept that our
culture continues to diversify. Cultural
competency, especially in healthcare, is the ability to
understand and respond effectively to the cultural and linguistic
needs of patients or clients. Implied is the acceptance and
tolerance of different backgrounds and their associated traits,
beliefs, etc., and absence of prejudice against unfamiliar
cultures. Learning to value diversity and being open-minded about
other cultures are key characteristics of cultural competency. A
culturally competent professional recognizes and understands the
differences in his or her culture and the culture of the patient
or client. Therefore, it is no wonder that cultural competency is
a current buzzword in health care.
Cultural competency is a process
that occurs along a continuum. At one end of the continuum is
cultural destructiveness and at the other end is cultural
proficiency. The chart below was developed by the National Center
for Cultural Competence in 1999.

According to the University of Michigan Health System, the steps
involved in developing personal cultural competency are as
follows:
- Recognize your own personal cultural biases and
preconceived ideas/opinions;
- Desire to learn about and become involved with people
from diverse cultures;
- Seek out and increase your knowledge about other
cultures; and
- Learn and develop multicultural communication and
counseling skills.
Along this journey to attain cultural proficiency, it is
important to understand the difference between stereotyping and
generalizations. Stereotyping
is an assumption that ALL people in a particular group think and
behave alike. Stereotypes are often judgmental and do not allow
for individual differences--for this reason, a stereotype is an ending point. For example, a
stereotype could be that "All white southerners eat pork, have
buttered grits for breakfast, and drink sugared tea." In contrast,
generalizations refer to
the trends or behaviors within a group, but with the knowledge
that further information is needed to determine if the
generalization applies to this particular person. Therefore,
a generalization is a starting
point. An example of a generalization-based questions is asking a
Jewish client "Do you follow traditional Jewish dietary laws?"
This question provides a starting point to work from rather than
stereotyping that all Jewish clients follow traditional dietary
laws.
Keep in mind that just as individuals within a cultural group are
unique, so are their diets. For example, not all
Japanese-Americans like wasabi. Thus the emphasis should be on
seeing the patient or client as an individual, which is also known as
patient-centered care. Providing patient-centered care can prevent
bias, prejudice, and stereotyping on the part of healthcare
providers from contributing to differences or disparities in care.
After all, the connection with the patient or client is the most important component.
According to the National Center for Cultural Competence, cultural
competency in healthcare is paramount for fostering more favorable
clinical outcomes, results in positive and rewarding interpersonal
experiences, and promotes patient or client satisfaction. In order
for health care to be successful, services must be received and
accepted. The real benefit of cultural competency is improved
outcomes. Cultural competency is NOT an optional skill to learn,
but rather a necessity.
In order to deliver culturally competent care, health care
providers should understand: beliefs, values, traditions and
practices of a person's culture, family structure and the roles
within the family in making decisions, health-related needs of
individuals, families, and communities, cultural beliefs about
health and etiology of diseases, cultural beliefs about healing
and disease treatments, and attitudes about seeking help from
health care providers.
The dominant American cultural paradigm is largely derived from
Anglo-American heritage and places high value on individualism,
privacy, personal responsibility and control. The "culture" of
healthcare in the U.S. reflects Anglo-American values, many of
which include being time oriented, focused on disease management
and treatment, and dedicated to preserving life at any cost. These
values are often in direct opposition of the values of many
traditional cultures, which often believe that fate, God or other
supernatural factors determines a person's destiny and directly
influences their health and family almost always includes extended
family, who commonly participate in the decision-making,
especially regarding health care.
When my colleague, Amber, was a dietetic intern, which means
she had completed her Bachelor's degree in nutrition but was
required to complete a one-year internship and pass a national
exam before she could use the title of Registered Dietitian,
she interned at a hospital where about 70% of the patients
were Vietnamese. She covered the cardiac unit, and the first
nutrition education that she provided was with a patient who
primarily spoke Vietnamese. The nurse was their translator as
she was from Vietnam. The nurse was kind enough to let Amber
know that when giving dietary instructions it would be
perceived as disrespectful to give the instructions without
the family present. Amber agreed to return when the family was
present.
Like language, food
distinguishes one culture from another. A culture is strongly
identified with its foods, and it's food preferences will out last nearly any other
cultural practice. After all, what could be more culturally
defining and also unifying than diet? Persons of all cultures
today expect space to be made for their cultural norms, and
individuals who accept the United States as their new home,
although they may adopt U.S. portion sizes and fast-food culture,
typically maintain many of their own cultural food practices. In
order to positively impact the diet and health of a person or
family from another culture, one must understand their culture,
their communication style, values, and health beliefs. By
understanding these cultural aspects institutional food services
can work on including a variety of ethnic foods that are
reflective of their client base and nutrition counseling
interactions can incorporate familiar cultural foods.
The images below were taken at Papa's Soul Food Kitchen BBQ in
Eugene, OR. The menu includes foods some Americans would consider
to be unique or strange, such as jerk chicken, southern fried
snapper, collard greens, black-eyed peas, and sweet tea.


A good starting point for learning about cultural, ethnic and
religious food customs is to be able to access the nutritional
composition of many traditional foods.
A handy resource is the Oldways
Preservation Trust website. The mission of Oldways is an
internationally-respected non-profit, changing the way people eat
through practical and positive programs grounded in science,
traditions, and delicious foods and drinks. It is best known for
developing consumer-friendly health-promotion tools, including the
well-known Mediterranean Diet Pyramid.
The Mediterranean, Latino, African, Asian,
and Vegetarian diet pyramids can be found on the Oldways
website.
The packet will ask you a few questions that will require you to
check out the Heritage Food Guide Pyramids in the link above.
Starting next week, Week 2, you will analyze the nutritional
status of individuals from different racial, ethnic, and/or
religious group and life cycle stages. The cuisines that will be
discussed for each racial, ethnic, and/or religious group will
include the following:
- Vegetarian cuisine
- Food customs of religious cultures
- Native North American Indian cuisine
- Japanese cuisine
- Asian Indian cuisine
- Southeast Asian cuisine
- Chinese cuisine
- Soul food
- and potentially Caribbean cuisine
Based on what we've discussed about the importance of cultural
competence we all must continually seek out opportunities to
develop culturally competent skills. Some of the ways in which you
can do this are listed below:
- Explore the media. Read books, magazines, and newspaper
articles, and explore Web sites. Watch movies, videos and
television programs that pertain to other cultures and are
ideally targeted toward immigrant groups and non-native
speakers.
- Arrange cultural encounters. Attend fairs and religious
events. Go to restaurants and ethnic markets. Look for
opportunities to socialize with individuals from the target
culture.
- Take a walk down the grocery store's "ethnic foods" aisle
for a cursory lesson in diet diversity or visit local "ethnic
food" markets.
- Seek information on acceptable behaviors, courtesies,
customs, and expectations from a cultural expert that can help
you prepare for interactions and interpret actions.
- Walk or drive through communities to identify where
people gather, what types of stores and restaurants are
available, what is being advertised in windows, and how often
you hear the native language spoken.
- Visit community organizations to learn about a particular
cultural group, such as schools, block associations, senior
citizen's groups, and women's clubs.
- Many cultural groups have Web sites were you may find
chat rooms, advertisements, marriage brokers, lists of mail
order places for ethnic foods, and descriptive information
about food practices.
- Attend professional development and training classes or
group discussions.
- Take language lessons.
- Travel.
Below are a few images taken at a Japanese-American Lantern
Festival in Eugene, Oregon.



One consequence of not attaining cultural competency can be seen
in the multitude of healthcare
disparities that exist in the United States. A healthcare
disparity occurs when a segment of the population bears a
disproportionate incidence of a health condition or illness. A
segment of the population can include gender, race, ethnicity,
education or income, disability, living in rural localities, or
sexual orientation.
In the U.S. there are four historically under-represented people
groups, African Americans, Native Americans/American Indians,
Latinos, and Asian Americans/Pacific Islanders. (Sound familiar to
the categories used in the most recent census?) In general, there
is a higher incidence of certain cancers, cardiovascular disease,
diabetes, obesity, and mortality in these population groups
compared to non-Hispanic whites.
The following list includes some of the most common causes of
healthcare disparities in the U.S.
- socioeconomic status (lower education and income levels)
- lack of insurance
- culture
- access to and utilization of quality health care services
- discrimination, racism, and/or stereotyping
- physical environment (e.g. housing conditions)
The following is an example of a healthcare disparity:
- English-proficient Hispanics were about 50% more likely
to report receiving advice on physical activity, as compared
with limited English-proficient Hispanics, after controlling
for health insurance coverage and number of visits to a
physician during the last year. Sex, age, region of residence,
level of education, annual family income, and smoking status
were not significantly associated with receiving physical
activity and/or dietary advice (Limited English Proficiency Is a Barrier to Receipt
of Advice about Physical Activity and Diet among Hispanics
with Chronic Diseases in the United States by
Lopez-Quintero C., Berry E.M., Neumark Y., JADA, October
2009, 109:10, Pages 1769-1774).
Unfortunately, in today's fast paced life the health care
system is not immune to time pressures. The Institute of Medicine,
in its report Unequal Treatment: Confronting Racial and
Ethnic Disparities in Health Care, cast a spotlight on
time pressure in the clinical setting to eliminate stereotyping
and other uncertainties that could have a negative effect on
quality of care. “In the process of care, health professionals
must come to judgments about patients’ conditions and make
decisions about treatment, often without complete and accurate
information. In most cases, they must do so under severe time
pressure and resource constraints... [leading to] those factors
identified by social psychologists as likely to produce negative
outcomes due to lack of information, to stereotypes, and to
biases.”
The Office of Minority Health of the US Department of Health and
Human Services (HHS), in conjunction with the Agency for
Healthcare Research and Quality, established National
Standards
on Culturally and Linguistically Appropriate Services
(CLAS), a collection of 14 mandates, guidelines, and
recommendations designed to eliminate racial and ethnic health
disparities. The idea behind the CLAS system is that better
communication leads to better adherence to medications and
lifestyle changes, which leads to improved health status, which
leads to less use of emergent care services and less frequent
hospitalizations
III. Nutrition Review
This week we will spend some time reviewing the basic principles
of nutrition. It might be helpful to dust off your FN 225 and/or
FN 105 notes and textbook, if you still have them, especially if
it's been awhile since you've taken the course. Don't forget to read chapter 1 of your textbook
this week too, which will provide you with a nutrition and health
overview. (Note that since your textbook was published in
2009, the sections related to Healthy People 2010,
Dietary Guidelines 2005, and MyPyramid are now Healthy People
2020, Dietary Guidelines 2010, and MyPlate. I have included
updated information in the lecture below.)
A. Health and Healthy People
The World Health Organization
(WHO) defines health as a "state
of complete physical, mental and social well-being, not merely
the absence of disease or infirmity."
Healthy People 2020 comprises the
Nation's comprehensive health objectives and stresses the need
to provide culturally competent, community-based health care
systems in order to address health disparities among different
segments of the population. Healthy People 2020 is considered to be
a health curriculum for the nation.
The "Overarching Goals" of Healthy
People 2020:
- Attain
high-quality, longer lives free of preventable disease,
disability, injury, and premature death.
- Achieve health
equity, eliminate disparities, and improve the health of
all groups.
- Create social and
physical environments that promote good health for all.
- Promote quality
of life, healthy development, and healthy behaviors
across all life stages.
B. From Dietary Reference Intakes to
MyPlate
-
DRI (Dietary
Reference Intakes): umbrella term for four possible
values that set nutrient intake standards for people
living in the U.S. and Canada (Dietitians commonly use DRI values when
determining the estimated needs of the patients they are
assessing, such as how many grams of protein one needs
per day. DRIs are also used for menu planning and
analyzing 24 hour recall data to prevent over or under
nutrition.)
-
Dietary Guidelines
for Americans 2010 and MyPlate are tools that help us translate scientific
research into everyday food choices.
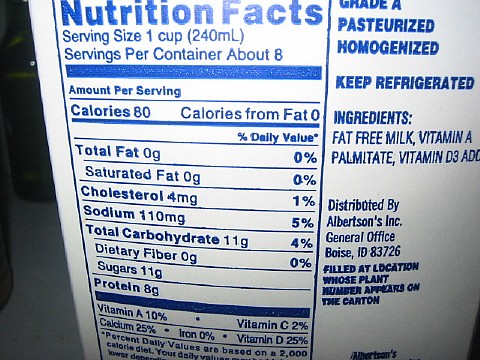
C. Food Labels
-
DV- Daily
Value: food labels do NOT use the DRI values, but a
separate set of suggested daily intakes of calories and
selected nutrients (*We are going to say that the "magic"
%Daily Value is 10%.
In other words, we will consider a food a good source of a
nutrient if it has 10% or greater of the DV for that
nutrient per serving.*)
- If you need some additional resources to answer the
questions below check out the following links:
- Remember the following energy-yielding nutrients
(macronutrients) and their calorie content:
- Carbohydrates: 4 calories
per
gram
- Protein: 4 calories
per
gram
Use the food label image
above to answer the questions in your outline.
IV.
Chapter
1: Nutrition & Health Overview
Read Chapter 1
in your textbook and answer the questions in your outline.
Choose one of the online nutrition resources
below and answer the questions in your outline.
End of Week 1 Unit Preparations
After filling in ALL of the blanks to the
questions in your outline, go to the "Unit 1 Study
Questions" under Week 1 in Moodle to submit your answers.
(Note: If you take the
quiz after the due date, please send me a message. It will
probably not
be graded
until you do that as I
may not realize it was done. I can do this ONE time.)